Douglas F. Milam M.D.
Urologic Surgery
- Home
- About Us
- Surgical Procedures

- Evaluation of Voiding Dysfunction
- Patient Information
- IPSS-AUA Symptom Score
- Sexual Function Questionnaire
- Deactivate a Urinary Sphincter
- VPEC
- Overnight Surgical Stay
- Post-operative Instructions Urethral Stricture Repair
- Post-operative Instructions Penile Implant
- Post-operative Instructions Artificial Urinary Sphincter
- Post-operative Instructions Placement of Male Sling
- Post-operative Instructions Penile Curvature Repair
- Post-procedure Instructions Vasectomy
- Mechanism of Erection
- Statement on Urologic Pain
- Schedule a Consultation
- Directions
- Urologic Images
- Web References
Male Continence Procedures
ARTIFICIAL URINARY SPHINCTER (AUS)
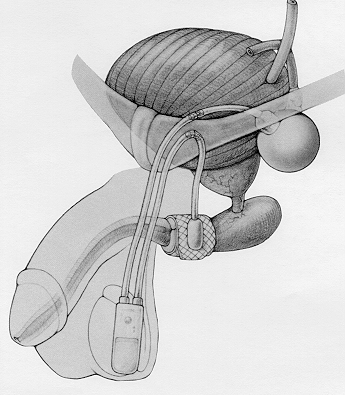
Artificial urinary sphincter (AUS) diagram. All parts of the device are implanted inside the body. The pressure regulating balloon, urethral cuff, and pump are shown here connected by tubing.

This photograph shows the three parts of the AUS. Shown from left to right are the urethral cuff, an empty pressure regulating balloon, and the pump. Different sizes of urethral cuffs are used depending on the measured circumference of the patients urethra. The pressure regulating balloon is filled with about 23ml of saline (salt water) during the operation. The pressure regulating balloon generates a carefully selected amount of pressure causing the urethral cuff to gently squeeze the urethra. That is how an AUS improves continence. The pump which is placed in a dependent portion of the scrotum is shown on the right. Compression of the bottom half of the pump causes fluid to be withdrawn from the urethral cuff, opening the urethra and allowing the patient to urinate. The urethral cuff and the pump are antibiotic coated (yellow color) to minimize the risk of infection. The pressure regulating balloon cannot be antibiotic coated at this time due to manufacturing considerations.




Once the plane has been developed between the urethra and the underlying corporal body, we measure the circumference of the urethra in order to select the proper size urethral cuff. In this case, the urethra measures almost 4 3/4 centimeters. A 5cm cuff would be used in this case. This urethra is more normal than many we see. Prior surgery or radiation therapy often leads to loss of urethral tissue (atrophy). In severe cases of atrophy we often place the urethral cuff behind the next layer backing the urethra (transcorporal placement) instead of the standard placement shown immediately below.

The artificial urinary sphincter cuff is shown here surrounding the urethra. This is a typical placement where the urethra is circumferentially separated from surrounding tissue for about 1.5 centimeters. The cuff is passed around the urethra and the snap connection is made at the tubing take-off. The next step of the operation is to rotate the tubing take-off to the left (patients right) and to bring the tubing to the upper incision where all tubing connections are made.
![]()
Transcorporal AUS Cuff Placement: This extreme close-up photograph shows the urethra running top to bottom in the center of the photo. The patient has very severe atrophy (loss of tissue) of the urethra due to prior surgery and radiation therapy. In selected cases like this we may choose to perform a transcorporal cuff placement. This provides an additional tissue layer behind the urethra in an effort to minimize the chance of erosion of the cuff into the compromised urethral tissue. The two purple marks lateral to the urethra on the corporal bodies indicate the site of the incisions. We will open the corpora in order to create a tunnel under the urethra within the corporal body.
![]()
The right angle clamp has been passed within the corporal body, but immediately behind the urethra. This provides an extra layer of tissue to minimize the risk of urethral cuff erosion in patients who have experienced substantial urethral atrophy. The clamp grasps a flange on the cuff made for this purpose and passes the cuff around the back side of the urethra. The snap mechanism shown two photographs above completes the urethral cuff placement.

Here is a view looking through a cystourethroscope into the urethra of a patient with an AUS. The cuff of the AUS completely encircles the urethra and is only a few millimeters under the urethral lining. In this case the cuff is 50% closed. The urethral channel can be seen as the dark area on the other side of the cuff. It is very important to fully empty the urethral cuff before attempting to pass a catheter into the bladder.

This is a view of the outline of the AUS pump through the scrotal wall 4.5 months after the device was implanted. The AUS urethral cuff remains closed until the pump bulb is compressed. Pressing the pump bulb forces the fluid (saline, salt water) in the cuff through the pump and into the pressure regulating balloon. With the cuff decompressed, the patient can urinate normally. The urethral cuff refills under pressure in 60-90 seconds restoring continence.
The AUS can be deactivated (turned off) by fully compressing the pump bulb 2-3 times and then quickly and firmly compressing the deactivation button. The pump bulb should remain at least 1/2 empty. If each side of the pump bulb has an indentation (dimple) after 2 minutes the device can safely be considered deactivated. Click here for detailed instructions of how to deactivate the AUS.
MALE SLING
A male sling is a synthetic hammock surgically implanted to support the urethra.

This overview slide shows the sling passing through the holes in the pelvic bone (Obturator Foramen) and passing under and supporting the bulbar urethra. A sling does not add sphincter function to the urethra, but hopefully allows the patients own sphincter muscle to function more effectively.

The male sling is implanted through a small incision in the perineum under the scrotum. We incise the overlying tissue layers until the urethra is encountered (center of the photo). Fibers from the perineal body attach to the urethra. The most distal (downstream on the urethra) of these fibers have been removed and a purple mark was placed in that location. This is the location where the sling will be implanted.

Synthetic Mesh of a bone anchored male sling implanted in the perineum. Several layers of tissue are closed over the sling in addition to the skin layer.
INTERSTIM
Treatment for urinary frequency, urgency, and urinary retention

Interstim is a technique where a low amplitude electrical current is used to neuromodulate the nerve signals coming from and going to the bladder. It is performed as a two stage procedure.
On each side of the back of the pelvis there are 4 holes in the bone, or foramina. Here we see needles inserted into the third foramen on both right and left sides. A special wire is passed through the needles into the region of the nerves. Once testing is complete, we remove the needles leaving one or both wires in place. The wire is connected to a special cell phone sized generator box that the patient wears for a one week trial. Interstim is useful for urinary urge incontinence, urinary urgency and frequency, and urinary retention.

If the one week Interstim test period is successful, a permanent generator can be implanted in the operating room. This photo shows an Interstim II device being implanted. This generator is connected to the lead that stimulates the nerves coming to and from the bladder and has a battery life of about 3 years.