Douglas F. Milam M.D.
Urologic Surgery
- Home
- About Us
- Surgical Procedures

- Evaluation of Voiding Dysfunction
- Patient Information
- IPSS-AUA Symptom Score
- Sexual Function Questionnaire
- Deactivate a Urinary Sphincter
- VPEC
- Overnight Surgical Stay
- Post-operative Instructions Urethral Stricture Repair
- Post-operative Instructions Penile Implant
- Post-operative Instructions Artificial Urinary Sphincter
- Post-operative Instructions Placement of Male Sling
- Post-operative Instructions Penile Curvature Repair
- Post-procedure Instructions Vasectomy
- Mechanism of Erection
- Statement on Urologic Pain
- Schedule a Consultation
- Directions
- Urologic Images
- Web References
Mechanism of Erection
Mechanism of Erection and Penile Implant Function
Men often ask about the particulars of the erectile mechanism. They wonder what changed to make it difficult or impossible for them to have normal erections. We now know that the erectile mechanism is very complex and involves different types of nerves, arteries carring blood to and through the penis, veins returning blood to systemic circulation, and a very complex control mechanism where the nerves join the small arteries. The end result of the normal erectile mechanism is that blood flows under pressure into the two erectile bodies of the penis. These erectile bodies, or corpora cavernosa, run the length of the penile shaft and continue inside the body to attach onto the pelvis bone. Normal erectile bodies are tough, but contain substantial elastic fibers which allow them to stretch up to a certain limit. Blood flowing into the erectile bodies under normal blood pressure causes them to stretch and become rigid. The firmness of penile erection results from the stretch of the erectile bodies. When a man has a penile implant, the implant cylinders are placed inside the erectile bodies. Pumping saline into the cylinders merely mimics the normal process of filling the erectile bodies under pressure.
Triggering Erection
Sexual thoughts from the cerebral cortex, nocturnal stimuli from the brain during REM sleep, and tactile (touch) sexual stimulation may trigger the pathway leading to penile erection. Nerve signals are carried through the spinal cord to the pelvic nerve plexus, a portion of which becomes the cavernous nerves of the erectile bodies, or penile corpora cavernosa. The pelvic plexus receives input from both the sympathetic and parasympathetic nervous immediately below the aortic bifurcation and courses to the pelvic plexus. Parasympathetic fibers originate in sacral spinal cord segments 2-4 and join the pelvic plexus. Discrete nerves carrying both sympathetic and parasympathetic fibers innervate the organs of the pelvis. Nonadrenergic noncholinergic (NANC) nerves also follow the pelvic plexus to join the smooth muscle that surrounds and controls penile artery diameter by secretion of nitric oxide into the neuromuscular junction. In 1982 Walsh and Donker demonstrated that nerves coursing posterolateral to the seminal vesicles and prostate and immediately lateral to the membranous urethra continue on to innervate the corpora cavernosa (1). These nerves are the ones that can easily be damaged during removal of the prostate or rendered nonfunctional by radiation therapy for cancer treatment. It is now known that branches of those nerves are the principal innervation of the neuromuscular junction where arterial smooth muscle controls penile blood flow. Nitric oxide and cGMP play a critical role in regulating penile blood flow (2). Much work over the past two decades has confirmed and expanded on our understanding of the erectile process. The typical erectile dysfunction (ED) patient produces and releases less than the normal amount of nitric oxide into the neuromuscular junction. In addition to cancer treatment, normal aging, vascular disease, spine disorders, and neurologic disease can decrease nitric oxide production at the neuromuscular junction and vascular endothelium.
Neuromuscular Junction Dysfunction
Nitric oxide is released from cavernous nerves causing activation of guanylyl cyclase within the erectile body. The figure below illustrates that there are several steps that, if not functioning properly, could impede erectile function. Generation of nitric oxide by the cavernous nerves and the vascular endothelium appears to be a critical trigger for the erectile mechanism. Further understanding of all the steps in the erectile pathway will likely implicate additional biochemical reactions as causing ED.
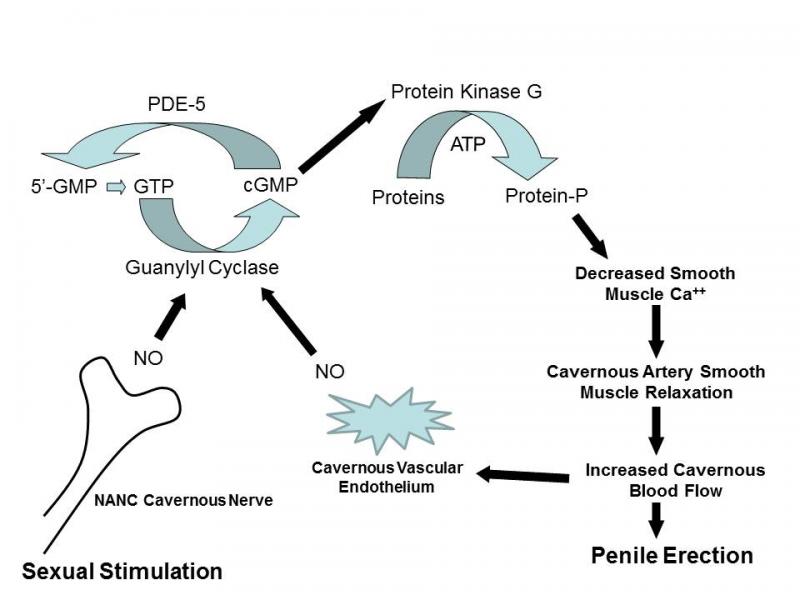
Place cursor on image to zoom in.
Penile Implant Function
Placement of a penile implant mimics the erectile mechanism by filling the penile erectile bodies under pressure with implant cylinders. A penile implant expands the patient's own erectile bodies until the inherent elastic limit of those erectile bodies is reached. At that point the penis is rigid and cannot expand further. The implanted cylinders would be capable of expanding further in almost all cases, but are limited in their expansion by the elastic limit of the patient's own erectile bodies. The photographs below demonstrate implant cylinders filled with saline in the unexpanded state and then stretched to their limit of expansion. These particular cylinders are from an AMS-700 LGX device. The orange color is from the rifampin and minocycline antibiotic coating.

Fully Deflated Implant Cylinders (Place cursor on image to enable zoom)

Unexpanded Implant Cylinders (Place cursor on image to enable zoom)

Expanded Implant Cylinders (Place cursor on image to enable zoom)
References:
(1) Walsh PC, Donker PJ: Impotence Following Radical Prostatectomy: insight into etiology and prevention. J Urol 128, 492, 1982.
(2) Kim N, Azadzoi KM, Goldstein I, et al: A nitric oxide-like factor mediates nonadrenergic, noncholinergic neurogenic relaxation of penile corpus cavernosum smooth muscle. J Clin Inves 88, 112, 1991.